I was kindly asked by the BMJ to write a piece for a “Head-to-Head” feature on EBM. Opposing me is the great Professor Darrel Francis, from Imperial College London and the National Heart and Lung Institute. The resolution at stake was the following: Does evidence-based medicine adversely affect clinical judgment? I took the affirmative, of course, and Dr. Francis the negative.
I’m very happy with it. I think it’s my best effort against EBM so far, but you can judge for yourself. Also, the BMJ is running a poll on this question. As it currently stands, my position is trailing 40% against 60%. However, given the pro-EBM indoctrination that has occurred over the last 30 years, I consider this to be a great victory!
How do we know that a treatment is bunk and doesn’t even need to be tested to be disproved?
A recent blog post by obesity expert Jason Fung ads fuel to the fire in the debate that opposes the standard-bearers of “science-based medicine” to those whom they view as practicing or promoting “pseudoscience.”
Fung attacked the perennial debunkers and his blog post prompted an immediate riposte by Dr. David Gorski.
Anish and I tried to sort through the controversy.
One of the most tiresome clichés in health care policy is the one that asserts that drug companies can mesmerize patients and doctors into using ineffective pharmaceuticals simply by way of an advertising campaign.
That claim was just made in the editorial pages of JAMA Internal Medicine and promptly spread via social media. The editorial purports that Allergan has managed to make vast sums of money in sales of Restasis, a dry eye treatment, even though the medication is demonstrably ineffective.
Anish and I examine the claim and find it seriously wanting. Here are the time stamps and the video (total watch time ~ 20 minutes):
A tweet catches Michel’s attention 0’30”
Anish summarizes the paper 1’30”
How do we know the drug “doesn’t work?” 4’20”
Anish presents his own market research…surprise, surprise, it’s Fake News! 9’05”
The “pharmascolds” are ideologues with no credibility 13’20”
In his judgment about Alfie Evans rendered February 20, 2018, Justice Hayden of the UK’s Royal Courts of London writes:
Crucial to the decision I am being asked to make is the need to ascertain, as accurately as it can be, the present level of Alfie’s awareness. Accordingly, I considered that an up-to-date MRI scan was a significant component in the broad sweep of evidence that was likely to inform this assessment.
Nowadays, it may seem obvious that an MRI should inform someone about another person’s level of consciousness because it is widely assumed that if consciousness is present, it must somehow be present “in the brain.”
I don’t have time now to discuss in detail why that view is not quite correct (you can sign up for my Philosophy of Nature and Man course if you have the urge to know!), but I am reminded of 2 amusing items.
I had a fun chat with Professor Darrel Francis on Evidence-Based Medicine. Here are some of the highlights:
1:18 – I throw down the gauntlet on EBM.
4:01 – Dr. Francis proposes the analogy of the chocolate-made washing machine spinner.
6:15 – My come back: overuse is not due to a lack of RCTs but improper incentives. Dr. Francis on the reception of ORBITA in the UK versus the US: “They don’t get angry!” EBM as tool for rationing.
11:20 – Dr. Francis: “How is it possible for there to be a single number that God has implanted in the coronary artery and revealed it to Nico Pijls…that tells us the risk/benefit ratio of stenting that patient?”
18:00 EBM and the placebo effect.
24:-30:00 – “Shared-decision making” is a sham.
31:00 – On the harm to clinical judgment: “I don’t mind the E, but I don’t want the BM in my practice!”
33:00 – Dr. Francis on “Bogle’s Demon” and “A vulnerable plaque is a plaque that has a stent in it.”
In our latest vlog, Anish and I discuss a thoughtful and well documented post by John Mandrola in which John rebukes the practice of using thrombolytic agents in acute stroke (“The Case Against Thrombolytic Therapy in Stroke.“). John’s post was itself prompted by a piece in the New York Times that is favorable to the use of the “clot-busting” treatment.
After posting our video, I was made aware of another post by an ER doc who, like John, is underwhelmed by the evidence in favor of thrombolytic therapy and, reflecting on the fact that numerous trials have tried to provide answers about the value of the treatment, asks “Why after 23 years do we still not know the answer?”
Of course, as readers of this blog know, my position is that RCTs are incapable of providing the answers that doctors seek (see, e.g., “The Devolution of Evidence-Based Medicine“).
Having expressed that opinion repeatedly here and on social media, I have been challenged by Professor Darrell Francis, professor of medicine at the UK’s National Heart and Lung Institute, and faculty at the Imperial College in London, to a debate (or, at least, a spirited discussion) that we will record and post on the channel.
This will happen in next week and should be really fun. Francis is a firebrand in the EBM movement, and has been principal investigator of several “game-changing” clinical trials.
Stay tuned, but meanwhile below is my discussion with Anish.
I am pleased to announce that Anish Koka and I will start a regular program on YouTube (and possibly later as a podcast) in which we cover topics of mutual interest in medicine and healthcare policy, including the latest scientific or policy brouhahas.
In our first episode, we discussed a recent editorial by John Ioannidis in which he considers the pros-and-cons of lowering the P-value threshold for statistical significance from the currently commonly accepted 0.05 to a lower threshold of 0.005. Bizarrely, Ioannidis thinks this could be a good idea (at least, that’s my interpretation of the paper. Anish gives him the benefit of the doubt).
Ioannidis, of course, made a big splash in 2005 with a paper entitled “Why most published research findings are false,” subsequent to which he rose to prominence beyond academia. (He was featured in a front-cover article in The Atlantic and in The Economist,and now leads the impressive-sounding Meta-Research Innovation Center at Stanford (METRICS). Here is his Wikipedia entry.) The meaning of false in that paper was not reproducible, so the paper marked a milestone in what is now commonly known as the “replication crisis.”
In the course of my conversation with Anish, I mentioned that the real crisis may very well be that the idea of “replication” as a standard of truth is not as sound as it may seem. In particular, I mentioned a recent editorial by Ioannidis and colleagues Goodman and Fanelli in which the authors acknowledge that replication can refer to different things, including replication of methods, replication of results, and—get this—replication of interpretation!
They give replication of interpretation the more technical sounding name of inferential reproducibility, which they define as “drawing out qualitatively similar conclusions from either an independent replication of a study or a reanalysis of the original study.” To Ioannidis et al., the lack of inferential reproducibility may be the “most important” and “under-recognized” dimension of the reproducibility crisis.
I’ll let you draw your own conclusions as to the significance of that definition, but if you want to hear our take on it, here it is:
On November 13, 2017, an epidemic of hypertension broke out and could rapidly affect tens of millions of Americans. The epicenter of the outbreak was traced back to the halls of the Anaheim, CA, convention center where the annual meeting of the American Heart Association was taking place.
The pathogen was released in a special 488-page document labeled “Hypertension Guidelines.” The document’s suspicious content was apparently noted by meeting personnel, but initial attempts to contain it with an embargo failed and the virus was leaked to the press. Within minutes, the entire healthcare ecosystem was contaminated.
At this point, strong measures are necessary to stem the epidemic. Everyone is advised not to click on any document or any link connected to this virus. Instead, we are offering the following code that will serve both as a decoy and as an antidote for the virulent trojan horse.Continue reading “How to stem the incipient epidemic of hypertension”
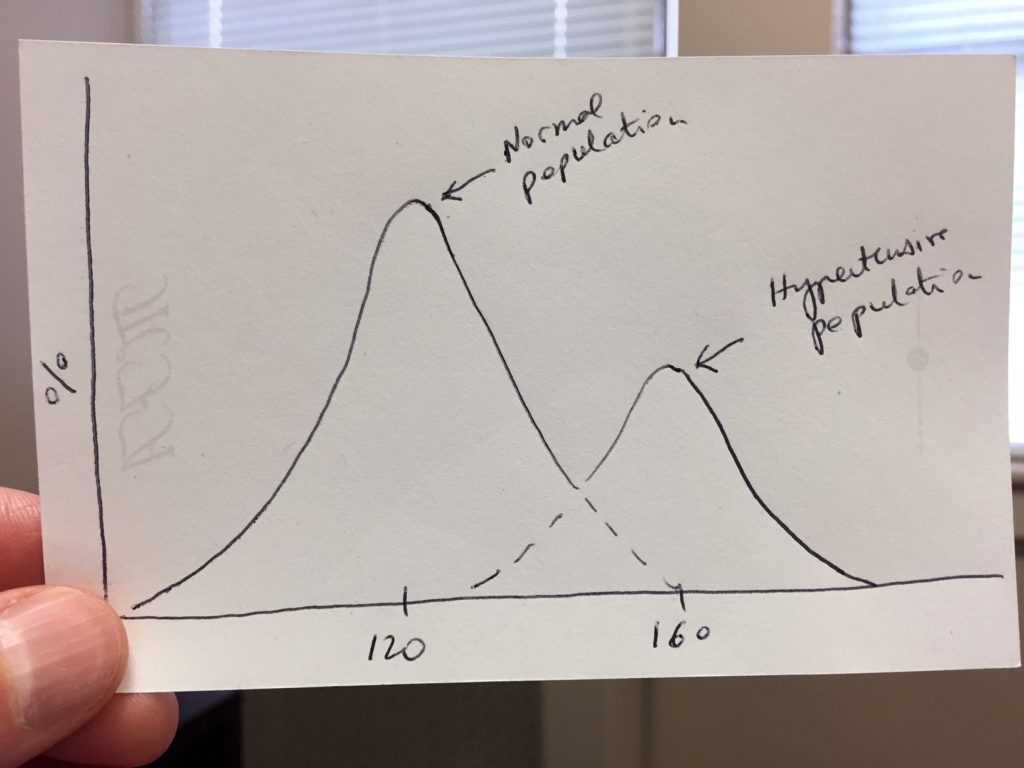
At the beginning of my new book, Socrates engages Geoffrey Rose to discuss one of the most fascinating conceptual questions regarding hypertension.
The question is the following: Compared to normal subjects, do hypertensive patients constitute a distinct population of patients? In other words, if we go out and measure the resting blood pressure of a large swath of the population and plot the numbers as a distribution curve, do we get two separate bell-shaped curves or just one?
A “2-peak” distribution of systolic BP
The answer to that question was the subject of an intense debate that began in the mid 1950s and lasted a couple of decades until it died down in the 1970s without any settled conclusion. Yet, an answer to that question is of critical importance not just for our understanding of hypertension, but for medical science in general and, by implication, for the direction of our healthcare system.Continue reading “Does Bergen, Norway, hold the key to the mystery of hypertension?”
I must admit that my initial reaction to the now famous study by Ashish Jha and colleagues—showing that female internists achieve slightly better 30-day inpatient mortality rates than male internists—was one of annoyance. “Here we go again,” I thought. “Data mining at the service of political correctness.” And I was pleased to read David Shaywitz reply to the study with a piece in Forbes aptly titled “When Science Confirms Your Cherished Beliefs—Worry.”