[This is the transcript of a paper I presented at the Austrian Economics Research Conference at the Mises Institute. I have included the slides below and you can hear the audio here. The title of the paper is “From reacting machine to acting person: a praxeological interpretation of the patient, his health, and his medical care.” For more info on praxeology, see my previous article here. I have split the presentation into two parts. This is a very condensed talk, covering a lot of ground, but I will elaborate on various points I make in the paper in the ‘progress notes’ section of this website over the next few days and weeks. Thank you for reading and for any feedback you might have.]
The elephant in the room in healthcare is that there is no precise definition of health. I believe that this ambiguity plays a major role in our perennial healthcare crises, and I am hopeful that Austrian insights can be helpful.
Here is the outline of my talk.
I will first identify the two dominant modes of thinking about health in modern Western societies. I will show that those conceptual modes are counterproductive to fostering health, both economically and medically. I will then propose a praxeological interpretation of health, and sketch the possible benefits and ramifications of that interpretation.
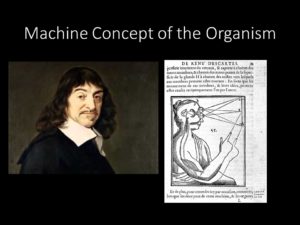 The dominant mode of thinking about health in Western societies owes its origins to René Descartes who, at the beginning of the scientific revolution, proposed the machine concept of the organism. Descartes’ proposal was a radical departure from pre-existing notions which were rooted in the idea that organisms have essences and natures. Instead, he proposed that every material body is an assemblage of tiny particles moving mechanically according to physical laws. In the case of plants and animals, God directs the laws and the motions. In the case of humans, the mechanical bodies are under the control of a separate human soul acting like a “ghost in the machine.”
The dominant mode of thinking about health in Western societies owes its origins to René Descartes who, at the beginning of the scientific revolution, proposed the machine concept of the organism. Descartes’ proposal was a radical departure from pre-existing notions which were rooted in the idea that organisms have essences and natures. Instead, he proposed that every material body is an assemblage of tiny particles moving mechanically according to physical laws. In the case of plants and animals, God directs the laws and the motions. In the case of humans, the mechanical bodies are under the control of a separate human soul acting like a “ghost in the machine.”
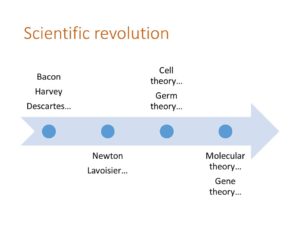 In the centuries that followed Descartes’ proposal, scientific discoveries began to lend credence to a machine concept of the body, however ill-defined that concept might have been, and, vice versa, the machine model facilitated further scientific discoveries. Laws of classical physics and chemistry were identified. Organisms were revealed to be made of basic material components that were increasingly well characterized, and these components were seen to act on each other according to physical laws to produce predictable biological behaviors. And certain diseases were recognized as being due to defects in components of the machine-like organism.
In the centuries that followed Descartes’ proposal, scientific discoveries began to lend credence to a machine concept of the body, however ill-defined that concept might have been, and, vice versa, the machine model facilitated further scientific discoveries. Laws of classical physics and chemistry were identified. Organisms were revealed to be made of basic material components that were increasingly well characterized, and these components were seen to act on each other according to physical laws to produce predictable biological behaviors. And certain diseases were recognized as being due to defects in components of the machine-like organism.
By the end of the nineteenth century, when healthcare systems were beginning to emerge, the machine model was widely adopted by scientists and was bearing much fruit in medicine.
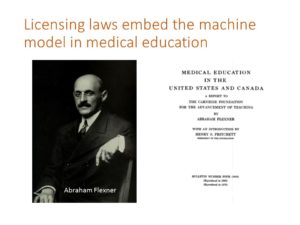 Now, there is nothing wrong with models, so long as they are understood to be models. But under the dual influence of ideological empiricism, which was widespread among prominent scientists, and social progressivism, which was flourishing in many Western nations at that time, medical licensing laws incorporated and embedded the machine model into medical education, turning it into a quasi reality.
Now, there is nothing wrong with models, so long as they are understood to be models. But under the dual influence of ideological empiricism, which was widespread among prominent scientists, and social progressivism, which was flourishing in many Western nations at that time, medical licensing laws incorporated and embedded the machine model into medical education, turning it into a quasi reality.
This is particularly well documented in the case of the United States, which saw an abrupt transition from a unique free market situation to a regulated healthcare environment in the 1910s. The transition was instigated at the behest of the Carnegie Foundation whose leaders were enthusiastic about the progressive idea of “scientific” management of social affairs. They entrusted Abraham Flexner to issue a report that was highly critical of the state of medical education for failing to systematically embrace scientific empiricism.
The Flexner report explicitly promoted the machine concept of the human body and, in the aftermath of its publication, educational and licensing reforms were enacted to prevent the operation of any medical school that did not embrace the proposals advanced by Flexner. If the body is like a machine, its care should only be entrusted to those who receive proper scientific training.
 The educational and licensing regulations of that period have dictated the modern medical school curriculum, a curriculum that has remained essentially unchanged since then: Entrance requirements mostly hinge on mastery of the physical sciences, and the curriculum begins with “building block” disciplines, then moves to more complex systems. With that constructivist approach, an understanding of the body is expected to emerge from the conceptual integration of parts into systems, as one would mentally construct the workings of a machine.
The educational and licensing regulations of that period have dictated the modern medical school curriculum, a curriculum that has remained essentially unchanged since then: Entrance requirements mostly hinge on mastery of the physical sciences, and the curriculum begins with “building block” disciplines, then moves to more complex systems. With that constructivist approach, an understanding of the body is expected to emerge from the conceptual integration of parts into systems, as one would mentally construct the workings of a machine.
Again, there is nothing inherently wrong with such a structure, unless our scope of understanding remains confined to it. To the extent that licensing laws and educational regulations privilege empirical knowledge over all other forms of knowledge, and to the extent that the hard sciences are considered foundational to the medical curriculum, the concept of health becomes difficult to articulate precisely within such a structure.
The notion of health necessarily pre-supposes certain ontological considerations regarding the human person, yet the empirical sciences precisely avoid such considerations. As a result, the concept of health is generally left undefined, while the machine model, seen as highly effective for the production of therapeutic advances, has become a de facto representation of the human body in medical circles.
 From that model of the human body, a certain understanding about health and disease emerges. If the body is viewed as a machine subject to disturbances, internal or external, then diseases are viewed primarily as objective dysfunctions, and health is simply the absence of disease. In fact, this is a common definition of health provided by standard medical dictionaries.
From that model of the human body, a certain understanding about health and disease emerges. If the body is viewed as a machine subject to disturbances, internal or external, then diseases are viewed primarily as objective dysfunctions, and health is simply the absence of disease. In fact, this is a common definition of health provided by standard medical dictionaries.
But neither the machine model nor the definitions of health and disease are firmly or explicitly considered valid or true. In fact, if examined, they are usually widely recognized as flawed or limited. Nevertheless, these have become operational definitions, given the empirical constraints imposed by the regulatory conditions for licensing and education.
 As we might expect, impelling the adoption of the machine model through educational and licensing regulations has had negative consequences.
As we might expect, impelling the adoption of the machine model through educational and licensing regulations has had negative consequences.
If health and disease are viewed as objective conditions to be ascertained by the physician, then the physician is put squarely in control, and patients are passive since their bodies are mere machines. This, of course, gives rise to medical paternalism which was particularly acute in the first half of the twentieth century. It also gives rise to an invasion of medicalization where, under authority from the medical community, increasing aspects of life are placed under the purview of the healthcare system. Medical authorities may also find opportunity to identify diseases that would not be apparent (or would not exist) under a different framework.
The view that health and disease are objective concepts also invites third parties to partake in healthcare delivery, namely, regulators and insurers.
Viewing healthcare as a purely technological endeavor, regulators wish to subject it to quality and safety oversight.
Viewing diseases as defects or dysfunctions in a machine, insurers—whether public or private—are tempted to think of medical illnesses as insurable events.
These errors account in large part for the endless bureaucratization and runaway cost inflation of healthcare.
And the machine model is self-fulfilling. Again, since only empirical methods are considered permissible to advance claims about health and disease, these methods limit our framework of understanding to only what is measurable. When health is not being “delivered” by the system according to accounting measures or measures of efficiency, more interventions are called for, and those interventions further mechanize care and reinforce the machine model of the human body.
 Now, clearly, there has been some backlash against a mechanical and reductionist concept of health in the last 50-60 years. The backlash began in part in response to the abuses of the eugenics movement, but also to other egregious abuses of a medical community empowered by licensing privileges and by technological means to cause great harm. Since then, alternative definitions have been proposed.
Now, clearly, there has been some backlash against a mechanical and reductionist concept of health in the last 50-60 years. The backlash began in part in response to the abuses of the eugenics movement, but also to other egregious abuses of a medical community empowered by licensing privileges and by technological means to cause great harm. Since then, alternative definitions have been proposed.
Chief among these alternatives is the definition of health offered by the World Health Organization in 1949 that health is “a state of complete physical, mental, and social well-being, and not merely the absence of disease or infirmity.”
While the WHO definition clearly acknowledges the subjective dimension of health, it has serious limitations.
 To begin with, by stipulating “complete well-being,” the WHO definition makes it hard to conceive of anyone as being healthy. It does not circumscribe the scope of medical care but, in fact, makes it limitless.
To begin with, by stipulating “complete well-being,” the WHO definition makes it hard to conceive of anyone as being healthy. It does not circumscribe the scope of medical care but, in fact, makes it limitless.
The definition also introduces the unclear notion of “social well-being” with which medical care is easily turned into a public health, or even a political activity.
And by defining health as “well-being,” the WHO definition, and others like it, appeal to an empiricist concept, namely, the idea of the self as a “bundle of experience,” as the philosopher David Hume put it. In this view, only the feelings and experiences of the person ultimately matter.
As a summary, we can remark that both concepts of health—the one that derives from the machine model and the one offered by the WHO—primarily consider the human being as reacting to changing conditions, rather as a person acting on the world to achieve chosen ends.
Part 2 follows here.
Great article, Michel!
In addition to the machine model, you might add the military model, as the two overlap.
Strangely, physicians rely on the set of things included in what philosophers call ‘intentionality’ in order to gather and communicate information about problems and treatments for the machine. Docs rarely notice the pervasive intentionality required to support their physicalist paradigm.
Great paper! I’m going to listen to the lecture now….
Best
Shawn
Thank you, Shawn! And you’re absolutely right…there is no escaping intention and teleology!
Michel